As clinicians, we’ve all faced the frustration of a restoration failing—an unexpected fracture, marginal gap, or patient dissatisfaction that undermines our hard work and impacts oral health. What if there were a material combining unrivaled strength with lifelike aesthetics, eliminating many of these common headaches?
It is Zirconia - a high-performance ceramic that addresses chipping, fit, and biocompatibility concerns without sacrificing the natural appearance your patients demand.
So, let’s compare zirconia vs other common dental materials. We’ll find out how zirconia compares to PFM, lithium disilicate, and metal alloys, which will help you pinpoint the ideal material for every clinical scenario and elevate your restorative outcomes.
Modern Dental Materials Overview
Step into your practice’s laboratory: Are you confident that today’s materials are meeting both your clinical demands and your patients’ aesthetic expectations? From tried-and-true metal alloys to cutting-edge ceramics, the landscape has never been more diverse—or more confusing. So let’s first know the modern dental materials in brief:
Zirconia
Zirconia used in dentistry is zirconium dioxide (ZrO₂) stabilized with yttrium oxide to prevent phase transformations during cooling and ensure structural integrity. CAD/CAM workflows allow milling of pre-sintered zirconia blocks, which are then sintered to achieve final dimensions and strengths up to 850–1,200 MPa.
Porcelain-Fused-to-Metal (PFM)
Porcelain-fused-to-metal crowns consist of a metal substructure with a porcelain overlay, combining durability with improved esthetics compared to all-metal restorations. They typically offer fracture resistance similar to full-metal crowns while providing an acceptable appearance for posterior and some anterior applications.
Lithium Disilicate (e.max)
Lithium disilicate is a glass-ceramic renowned for its high translucency and lifelike esthetics, making it ideal for anterior restorations and veneer. With flexural strengths of approximately 360–400 MPa, it offers good resistance to fracture but may require careful case selection in high-load posterior zones. Its monolithic fabrication and chemical bonding protocols simplify chairside workflows and reduce the risk of debonding.
Metal Alloys (Gold & Base Metals)
Metal alloys, including high-noble (≥60 % noble content), noble (25–60 % noble content), and base-metal (<25 % noble content) formulations, deliver unparalleled ductility and wear resistance. Their flexural strengths typically range from 500 MPa to 800 MPa, supporting long-span bridges and thin-section restorations without fatigue failure. Despite their mechanical superiority, the metallic color and patient demand for metal-free options often limit their use to posterior applications or implant abutments.
How Zirconia is Leading over All Other Dental Materials?
- Zirconia offers flexural strengths of 900–1,200 MPa, far surpassing lithium disilicate’s 360–400 MPa and PFM’s 80–100 MPa, translating to superior fracture resistance under heavy occlusal loads.
- Modern high-translucent zirconia formulations achieve enamel-like translucency comparable to lithium disilicate, making them viable for both anterior and posterior restorations.
- Yttria-stabilized zirconia is chemically inert and promotes excellent soft-tissue response, avoiding the allergic reactions sometimes seen with base-metal alloys.
- Although the upfront cost of zirconia restorations can exceed that of PFM, their exceptional durability and streamlined CAD/CAM workflows minimize long-term remakes and chairside adjustments, optimizing practice efficiency.
Zirconia vs Other Materials Comparison

Aesthetics Comparison
Zirconia’s advanced multilayer blocks achieve up to 42% translucency, closely mimicking enamel’s light transmission for lifelike anterior and posterior restorations. These zirconia formulations feature deep color gradients that prevent the “white-core” effect after adjustments, ensuring consistent shade even at minimal thicknesses. Lithium disilicate glass-ceramic crowns offer similar esthetic outcomes, with translucency parameters matching zirconia at clinically recommended thicknesses, making them the gold standard for veneers and anterior crowns.




Have you compared these materials’ translucency in your anterior cases?
Porcelain-fused-to-metal (PFM) restorations combine a metal substructure with veneering porcelain to balance strength and esthetics, but risk exposing opaque metal margins if gingival recession occurs. PFM’s porcelain layering process requires an opaque masking layer, which can limit final translucency and necessitate careful shade layering to avoid a frosty appearance.
All-metal crowns and base-metal alloys are entirely opaque, transmitting no light—a benefit when masking severely discolored teeth but a drawback for achieving natural translucency. Metal alloys’ inherent opacity ensures reliable esthetics in posterior applications, yet fails to satisfy patients’ growing demand for metal-free, tooth-like restorations.
High-translucent zirconia also reduces the appearance of gray margins, enhancing seamless gumline integration compared to PFM crowns. Conversely, lithium disilicate demands precise support in functional zones to prevent chipping, which can compromise its esthetic longevity under heavy occlusal loads. When selecting restorative dental materials for a crown , consider each patient’s smile line and tissue biotype—high translucency is critical in the esthetic zone, while posterior areas may prioritize strength over optical properties.
Strength & Durability Comparison
Flexural Strength
Zirconia exhibits exceptional flexural strengths ranging from 900 to 1,200 MPa, dramatically outpacing other ceramics and PFM veneers. Lithium disilicate’s flexural strength sits between 360 and 400 MPa, making it adequate for single-unit restorations but vulnerable under heavy occlusal forces. PFM restorations rely on a porcelain veneer layer with flexural strength around 80–100 MPa, which can chip if not fully supported by the underlying metal substructure.
Framework Durability
Though the metal frameworks in PFM crowns (gold or base-metal alloys) can reach strengths of 500–800 MPa, the veneering porcelain remains the weakest component and often dictates failure modes. Monolithic zirconia eliminates the porcelain layer, removing this common fracture point and virtually eradicating veneer chipping.
Preparation Requirements
Monolithic zirconia allows for minimal tooth reduction —preparation thicknesses as low as 0.6 mm—due to its high strength. Lithium disilicate requires at least 1.5–2.0 mm of clearance to achieve sufficient material bulk and avoid fractures. PFM crowns typically need 2.0 mm reduction to accommodate both metal coping and porcelain layering, increasing the risk of pulp insult in deep preparations.
Fatigue Resistance & Clinical Longevity
Zirconia’s superior fatigue resistance under cyclic loading reduces the risk of microcrack propagation and long-term failure, making it ideal for patients with bruxism or heavy occlusion. Lithium disilicate demonstrates good initial strength but lower fracture toughness (≈3.3 MPa·m¹ᐟ²), which can lead to fatigue fractures in high-stress posterior applications. PFM restorations withstand many years of service when correctly designed, but veneer fractures remain a recurrent complication, particularly in long-span bridges.
Clinical Implications
For posterior crowns, bridges, and patients with parafunctional habits, zirconia’s “ceramic steel” properties translate into predictable performance and minimal remakes. Lithium disilicate remains the material of choice for highly esthetic anterior cases but demands cautious case selection and protective occlusal schemes. PFM may still be selected for cost-sensitive cases where moderate strength and basic aesthetics suffice, provided veneer support and margin design are optimized.
Biocompatibility Comparison
Yttria-stabilized zirconia is virtually inert in the oral environment, promoting excellent soft-tissue integration and minimal inflammatory response around subgingival and supragingival margins. Studies show zirconia abutments wrapped in a thin fibrous capsule with collagen fibers oriented functionally, leading to stable peri-implant soft tissues and reduced bacterial adhesion over time. Have you noticed improved soft-tissue health and consistent gingival contours around zirconia crowns in your practice?
Glass-ceramic lithium disilicate also demonstrates high biocompatibility, with in vitro and in vivo research confirming it supports transmucosal applications without cytotoxic effects. Its chemical bonding capabilities result in a reliable marginal seal that minimizes microleakage and reduces bacterial colonization at the tooth–restoration interface.
In contrast, PFM restorations incorporate nickel-chromium or cobalt-chromium alloys that can elicit allergic reactions in a subset of patients, with symptoms ranging from mucosal inflammation to systemic hypersensitivity. While high-noble gold alloys reduce allergy risk, they still carry potential for galvanic currents and tissue discoloration over time.
Looking for a trusted lab partner? Get high-precision restorations from Advance Dental Export
Overall, zirconia’s metal-free composition and proven tissue compatibility make it the biocompatible material of choice for patients with thin gingival biotypes or known metal allergies. Combining biocompatibility with high strength and esthetics, zirconia minimizes the clinical complications related to soft-tissue irritation, ensuring predictable, long-term outcomes.
Cost Comparison
Understanding material costs alongside long-term practice efficiencies is critical—have you analyzed how your choice of crown impacts both patient investment and your clinic’s bottom line?
Zirconia Crowns Cost
Zirconia restorations in India typically range from ₹8,000 to ₹30,000 per unit, depending on brand, translucency, and warranty. Have you reviewed whether premium high-translucent blocks justify their higher fees through reduced remakes?
PFM Crowns Cost
Porcelain-fused-to-metal crowns are more budget-friendly, usually costing ₹5,000 to ₹15,000 per crown, with basic base-metal frameworks at the lower end and noble-metal alloys toward the higher end. Do you factor in potential veneer repairs or margin touch-ups when quoting PFM cases?
Lithium Disilicate (e.max) Cost
Glass-ceramic e.max crowns generally fall in the ₹10,000 to ₹20,000 range for a single anterior unit, balancing outstanding esthetics with moderate strength. Could strategic case selection—reserving e.max for low-stress zones—optimize both your outcomes and costs?
Metal Alloy Crowns Cost
Full-metal and metal-ceramic crowns using base-metal alloys or high-noble formulations span ₹5,000 to ₹15,000 per unit, offering exceptional durability but limited esthetics. Have you discussed alloy choices with patients who prioritize longevity over appearance?
Pro Tip: Conduct a quarterly audit comparing material costs, remake rates, and adjustment times to identify which crown type delivers the best long-term ROI for your practice.
Zirconia vs Other Dental Materials Comparison Table
| Criteria | Zirconia | Lithium Disilicate | PFM | Metal Alloys |
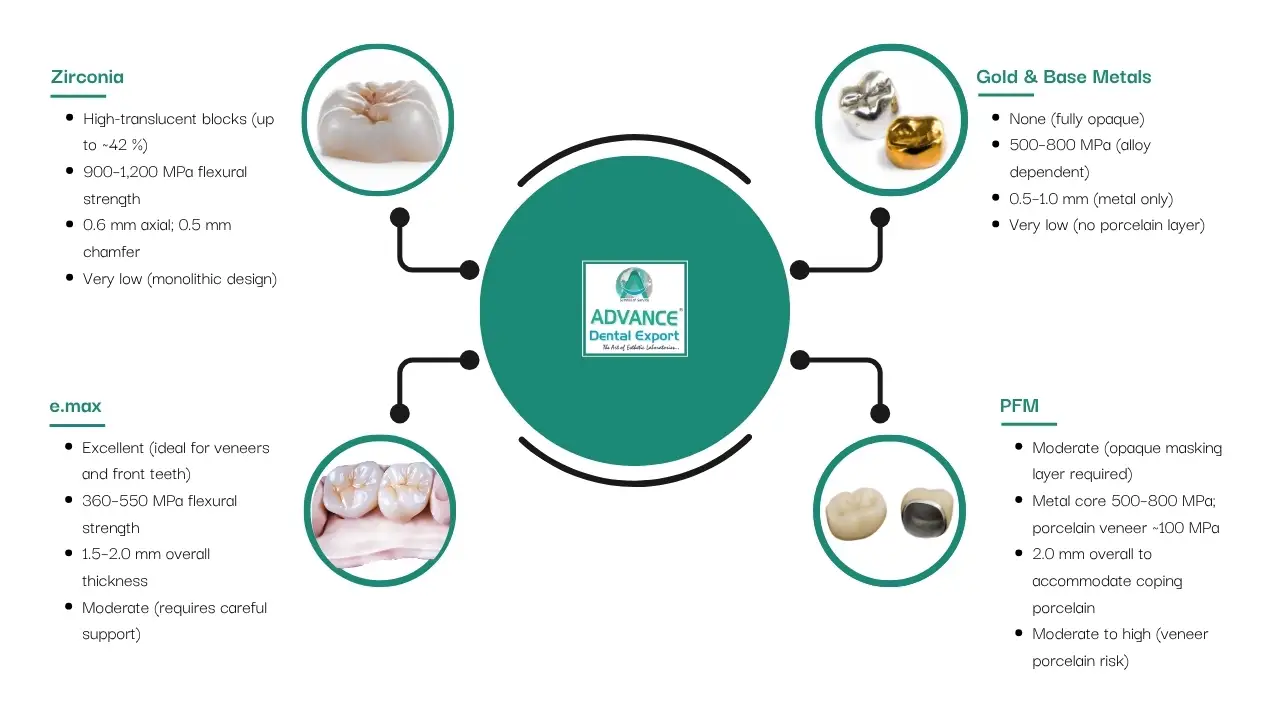
| Translucency | High-translucent blocks (up to ~42 %) | Excellent (ideal for veneers and front teeth) | Moderate (opaque masking layer required) | None (fully opaque) |
| Strength | 900–1,200 MPa flexural strength | 360–550 MPa flexural strength | Metal core 500–800 MPa; porcelain veneer ~100 MPa | 500–800 MPa (alloy dependent) |
| Minimum Prep | 0.6 mm axial; 0.5 mm chamfer | 1.5–2.0 mm overall thickness | 2.0 mm overall to accommodate coping + porcelain |
0.5–1.0 mm (metal only) |
| Chipping Risk | Very low (monolithic design) | Moderate (requires careful support) | Moderate to high (veneer porcelain risk) | Very low (no porcelain layer) |
| Biocompatibility | Excellent (metal-free; tissue-friendly) | High (glass-ceramic; strong bond to tooth) | Variable (nickel sensitivity risk in some alloys) | Variable (allergic potential) |
| Esthetics | Lifelike depth and color consistency | Superior depth and shade matching | Good, but risk of gray margins over time | Functional only; no shade matching |
| Cost (INR) | ₹8,000–₹30,000 | ₹10,000–₹20,000 | ₹5,000–₹15,000 | ₹5,000–₹15,000 |
| Ideal Use | Posterior crowns, bridges, and bruxism cases | Veneers, single-unit anterior crowns | Budget cases, moderate aesthetic demand | Long-span frameworks, posterior-only |
Conclusion
As you compare common dental materials with zirconia, I hope you make the right choice.
Zirconia stands out by combining exceptional strength, lifelike esthetics, and excellent tissue compatibility in one material. Its high fracture resistance and modern translucent formulations make it suitable for both anterior and posterior restorations, while its biocompatibility minimizes soft-tissue concerns. Although the initial investment is higher, streamlined digital workflows and fewer remakes deliver better long-term value.
By choosing Zirconia dental prosthesis from Advance Dental Export , you ensure reliable, natural-looking restorations that meet the highest clinical and patient-satisfaction standards.